
Featured Scientist: Andrew S. Huhn, Ph.D., MBA; Johns Hopkins University School of Medicine, Department of Psychiatry and Behavioral Sciences

Birthplace: Grand Ledge, Michigan
My Research: My research looks at different ways to improve treatment results for opioid use disorder. We are especially interested in finding ways to reduce sleep problems and stress with the goal of reducing unlawful drug use.
Research Goals: One goal is to evaluate the use of drugs as treatment for opioid use disorder. A second goal is to find a way to predict the risk of relapse for people who are in recovery for opioid use disorder.
Career Goals: My main goals are to grow my research portfolio and continue to train young scientists.
Hobbies: I like to read, play chess, and play sports with my kids.
Favorite Thing About Science: The results speak for themselves.
Scientist Upbringing: I didn’t want to become a scientist until I was in my mid-twenties. At that time, I was interested in helping patients with mental health. Only later I realized that there was a great need to improve treatment (broadly) and I saw science as an opportunity to study topics that I found interesting while working towards a larger goal of improving treatment for everyone.
My Team: As an Associate Professor, I have a team who implements my studies. I also work with a group of 5 professors who are all focused on opioids. We work with a group of 20 professors who are broadly interested in substance use disorders. There are also collaborations with professors outside of my department/school. While specific teams are formed for specific projects, we all work towards a common goal.
Organism of Study: Humans with opioid use and substance use disorders.
Field of Study: Behavioral Pharmacology
What is Behavioral Pharmacology? Behavioral Pharmacology is field research that focuses on how drugs affect the people who use them.
Check Out My Original Paper: “Latent trajectories of anxiety and depressive symptoms among adults in early treatment for nonmedical opioid use”
Citation: Ellis, J. D., Rabinowitz, J. A., Wells, J., Liu, F., Finan, P. H., Stein, M. D., II, D. G. A., Hobelmann, G. J., & Huhn, A. S. (2022). Latent trajectories of anxiety and depressive symptoms among adults in early treatment for nonmedical opioid use. Journal of Affective Disorders, 299: 223-232. https://doi.org/10.1016/j.jad.2021.12.004.
Research At A Glance: Opioids are drugs that can be used to treat pain. Unfortunately, many people in the United States misuse opioids for the “high” and to deal with mental health issues, like depression and anxiety. Unfortunately, over time, higher amounts of the drug are needed to achieve the same effects. As a result, people take higher doses. This increases the risk of overdose and death. These dangerous behaviors have resulted in a large increase in opioid dependence, loss of productivity, and death. In 2000, the opioid overdose death rate was 3 out of every 100,000 people. By 2020, the opioid overdose death rate was 21.4 out of every 100,000 people–an increase of 7.13 times!
In this research, the authors tried to find links between treatment for the misuse of opioids and symptoms of depression and anxiety. The authors also looked at people who were misusing opioids while also taking benzodiazepines. Benzodiazepines are a drug that causes deep relaxation and is sometimes prescribed by doctors to help with stress and anxiety, or to help people sleep. The authors wanted to see if the use of both opioids and benzodiazepines was related to symptoms of depression and anxiety. They also wanted to see if the use of both opioids and benzodiazepines was related to whether a person finished treatment. The authors found that many people who were in treatment for the misuse of opioids were also experiencing symptoms of depression and anxiety in the first four weeks of treatment. Some patients had severe symptoms, while others had milder symptoms. The authors found that patients who were experiencing persistent symptoms of depression were also more likely to leave treatment early, against the advice of their doctors. The authors did not find a relationship between symptoms of anxiety and the likelihood of leaving treatment early. The authors also found that symptoms of depression and anxiety were linked to the use of benzodiazepines with opioids. The findings of this research could lead to more helpful treatments for people struggling with opioid use disorder.
Highlights: To understand the relationship between treatment for the misuse of opioids and symptoms of depression and anxiety, the authors tracked symptoms of anxiety and depression in patients for the first 4 weeks of treatment. To measure this, the authors gave their patients surveys that asked questions about anxiety and depression.They then used a Growth Mixture Model (GMM) to analyze the data. GMM is a tool that allows researchers to track changes in data over time and identify groups based on the data. The authors used this method to track symptoms of anxiety and depression in the patients and to determine how symptoms changed over the course of 4 weeks. They then grouped participants based on the types of experiences they had.
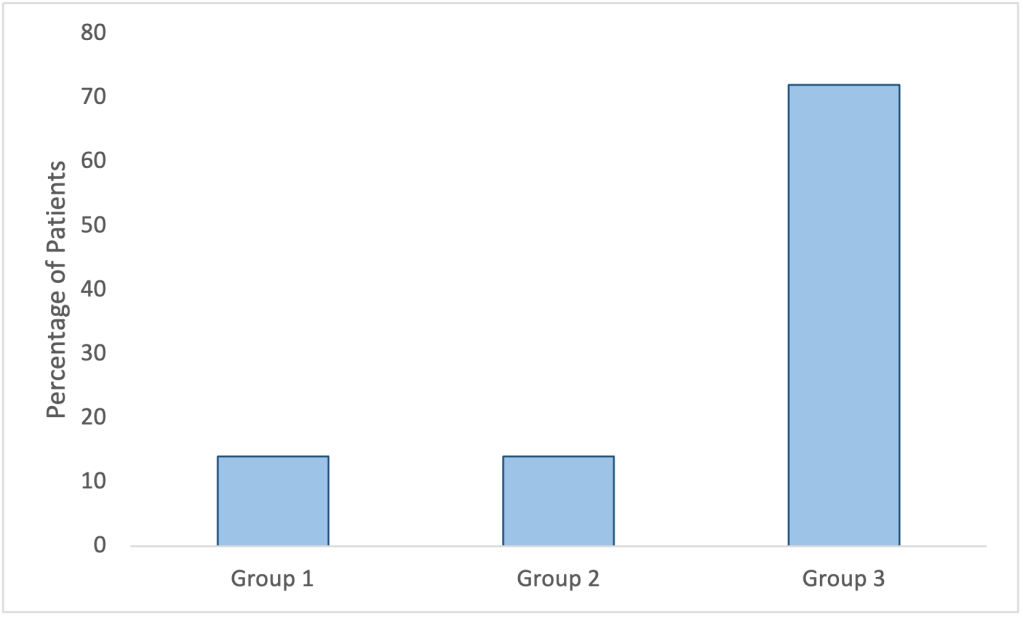
The authors found that patients fell into three groups based on their symptoms: 14% of the patients had average or intense symptoms of anxiety that didn’t go away during the first 4 weeks of treatment, 14% of the patients had intense symptoms that gradually started to go away, and 72% of the patients had mild symptoms that didn’t go away (Figure 1).
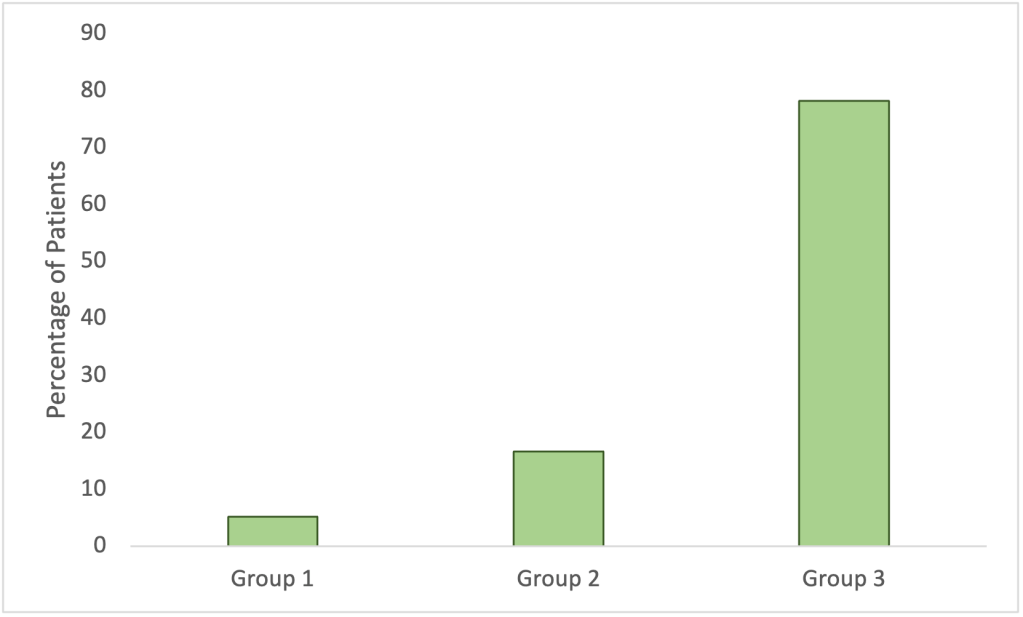
The authors found similar results for the patients with symptoms of depression: approximately 5% of the patients had intense symptoms that wouldn’t go away, approximately 16% had average symptoms that wouldn’t go away, and approximately 78% had mild symptoms that gradually started to go away (Figure 2).
While most of the patients had mild symptoms of anxiety and depression, there were some patients who experienced intense symptoms that didn’t go away with time. The authors found that female patients and patients who also used benzodiazepine may be more likely to have these intense symptoms. The same patients were also more likely to leave treatment early, against the advice of their doctors. The hope is that professionals can use these findings to create different types of treatment for patients with these symptoms to help them deal with their anxiety and depression.
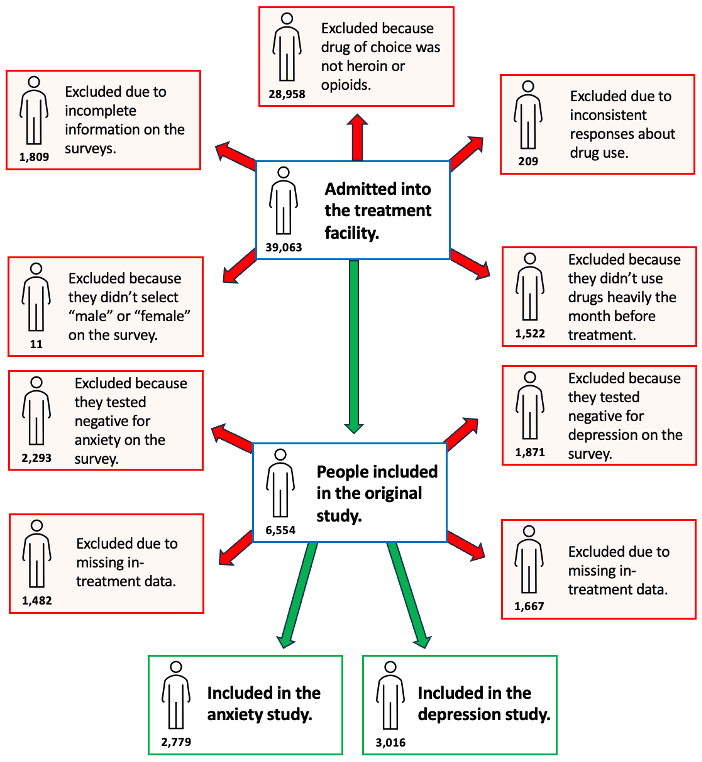
What My Science Looks Like: The participants for this research were originally recruited for a larger study monitoring the mental health and substance use behaviors of people in treatment centers. The larger study included over 39,000 people in inpatient and outpatient treatment centers. An important part of this study was identifying people who could help to inform the research. Figure 3 shows how the authors selected participants for this study.
The Big Picture: The misuse of drugs, such as opioids, is a problem that much of the U.S. is facing. Depression and anxiety, which are very common mental health challenges, have been linked to opioid use disorder. Learning about the populations most at risk for depression, anxiety, and drug misuse can help us create policies and programs that help change people’s lives. The findings of this research could lead to more helpful treatments for people struggling with opioid use disorder.
Decoding The Language:
Anxiety: Anxiety refers a feeling of fear, dread, and uneasiness. It could lead to sweat, feeling restless and tense, and a rapid heartbeat.
Benzodiazepine: Benzodiazepine is a type of drug used to relieve anxiety and insomnia (trouble sleeping). Benzodiazepines are also used to relax muscles and prevent seizures.
Dependence: Dependence refers to a physical reliance on a substance. In the context of this research, opioid dependence refers to a physical reliance on opioids. When someone is dependent on a drug it means that the body has begun to rely on the substance to maintain normal function. When it happens, people can begin to feel cold, and can experience shakes and tremors when they don’t have access to the drug.
Depression: Depression can be described as feeling sad, blue, unhappy, miserable, or down in the dumps. Most of us feel this way at one time or another for short periods, but some people can experience it persistently for long periods of time.
Growth Mixture Model (GMM): A growth mixture model is a statistical tool used to create groups based on collected data and to track changes in these groups over time. In the context of this research, GMMs were used to place participants into groups based on their symptoms of depression and anxiety. They were also used to see if patients experiencing these symptoms had reduced symptoms over time.
Opioids: Opioids are substances that are used to lessen pain and calm the nervous system. Examples of common opioids include oxycodone, codeine, and morphine.
Opioid use disorder: Opioid use disorder refers to a problematic pattern of opioid use that causes significant impairment or distress.
Relapse: A relapse occurs when an individual who is in recovery from drug or alcohol abuse returns to substance use.
Substance use disorder: Someone has a substance use disorder when their use of a drug negatively affects major aspects of their life.
Unlawful drug use: Unlawful drug use refers to the use of any controlled substance or dangerous drug that has not been legally prescribed and/or dispensed, or the use of a prescription drug which is not in accordance with the way it was prescribed.
Learn More:
A brief article from John Hopkins on the link between Opioid Abuse and Mood and Anxiety Disorders.
A YouTube video produced by the Centers for Disease Control (CDC) describing the Challenges of Opioid Use Disorder in Women.
An article from the CDC data on Death Rates Involving Opioids over time.
Synopsis edited by Dr. Rosario Marroquín-Flores, Texas Tech University, Department Biological Sciences and Dr. Jayme Walters, Utah State University, Department of Social Work.
Download this article here
Please take a survey to share your thoughts about the article!
Meet the Authors
Cassie Rees, junior at Utah State University

Cassie was born in Riverton, Utah, but currently resides in Logan, Utah while attending school. She is working towards obtaining a bachelors in social work with a psychology minor. Cassie enjoys music, traveling, hiking, and reading. She loves to work with people in any way possible! She has enjoyed working with special needs adults since graduating high school and worked as a camp counselor in Summer of 2022.
Amanda Meek, junior at Utah State University

Amanda is from Grantsville, Utah, but currently lives in Logan, Utah. She is currently working towards getting a bachelor’s degree in social work with a minor in American Sign Language (ASL). She loves to play the piano, solve rubik’s cubes, and paint. Amanda has loved working with children. After graduating, she wants to work in child welfare.
Simon Pitcher, junior at Utah State University

Simon is from Saratoga Springs, Utah. He’s working towards becoming a licensed clinical social worker and currently works, teaching skills to youth in the community. He loves playing pickleball and gets competitive with board/card games. He’s excited to become a dad soon, so that he can cover up his obsession with watching Pixar movies.
Zachary Swensen, junior at Utah State University
Zachary is from Wellsville, Utah. He is working towards a bachelor’s degree in social work with a minor in Spanish. Zachary loves to spend time outdoors, traveling, being with friends/family, and playing sports. After graduation, Zachary plans on obtaining a masters degree in social work and working in the mental health field.
